A 56 yo man with COPD has been receiving mechanical ventilation using volume assist control for the last 36hrs. His settings are: TV 6mL/kg RR 24 FiO2 0.4 PEEP 5. His ABGs have improved to: PO2 82mmHg, PCO2 42mmHg pH 7.37 and you switch him to a pressure support mode to provide a comparable tidal volume. However, he quickly becomes dyspneic. His ventilator graphics are shown.
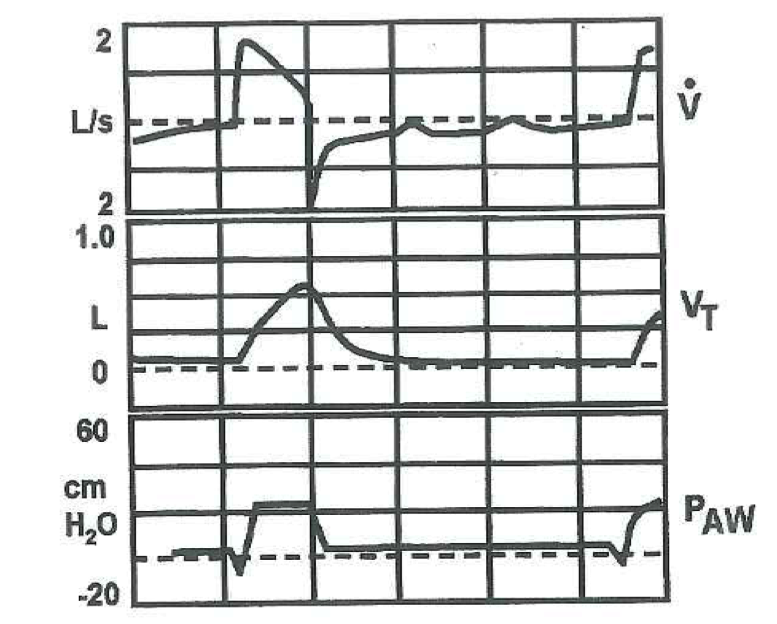
Explain the graphics.
Your next maneuver should be to:
A.Provide sedation and continue current ventilator settings
B.Switch from a pressure triggering to a flow triggering system
C.Add 5cm H2O additional PEEP and titrate up to improve triggering
D.Switch to the synchronized intermittent mandatory ventilation (SIMV) mode with a backup rate of 8/min along with the pressure support
E.Return to volume assist control with backup rate of 6/min
I think patient was on RR of 24 when he was on A/C which puts him at risk of Auto PEEP and air trapping . when he was switched to pressure support he was trying to trigger a breath but was faced with his PEEPi.
usually in obstructive disease we overcome the auto peep by lowering tidal volume or by lowering the RR or both to allow more time for the expiratory phase, however there is one role for applied PEEP in obstructive disease patients when PEEP can serve as an inspiratory threshold load ( usually 75 to 85 % of the auto peep ) to help the patient trigger a breath.
This is better explained in Murray and Nadal mechanical ventilation section.
The reference from a study in 1990.
http://www.ncbi.nlm.nih.gov/pubmed/2405757
And another study from 1997:
http://www.ncbi.nlm.nih.gov/pubmed/?term=Applied+PEEP+reduces+the+inspiratory+load+of+intrin
I think the answer to the question is C .